Congenital aortic valve dysplasia
kən-ˈjen-i-tᵊl ˈā-ˌȯr-tik valv dis-ˈplā-zh(ē-)ə
Also known as: Aortic valve malformation, Congenital aortic stenosis
At a Glance
What is Congenital aortic valve dysplasia?
Congenital aortic valve dysplasia is a heart condition present at birth where the aortic valve is malformed. This condition primarily affects the cardiovascular system, specifically the heart and its ability to pump blood efficiently. It is caused by abnormal development of the valve during fetal growth, which can lead to narrowed or obstructed blood flow from the heart. Over time, this can result in increased strain on the heart and potentially lead to heart failure if not managed. Early symptoms may include difficulty breathing, fatigue, or poor growth in infants, while later symptoms can involve chest pain or fainting. Early diagnosis is crucial to manage the condition effectively and prevent complications. The condition can impact family life by necessitating frequent medical visits and potential surgical interventions. Prognosis varies depending on the severity of the dysplasia and the success of treatments. Daily life for affected individuals may include activity restrictions and ongoing medical monitoring. Treatment options may involve medication or surgery to repair or replace the valve. With appropriate care, many individuals can lead relatively normal lives. Support from healthcare providers and family is essential for managing the condition effectively.
Medical Definition
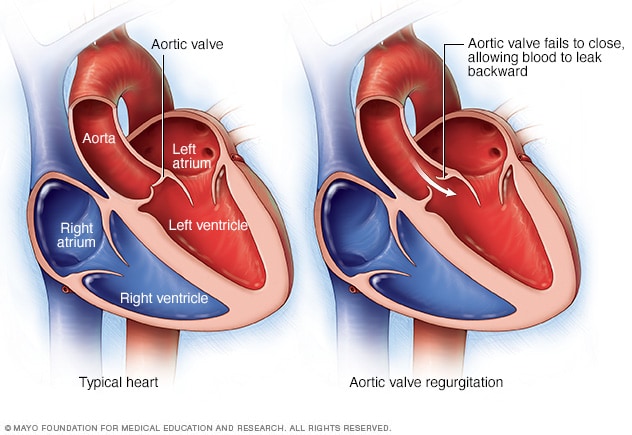
Congenital aortic valve dysplasia is characterized by the abnormal development of the aortic valve, often resulting in a bicuspid or malformed valve structure. Pathologically, this can lead to stenosis or regurgitation due to improper valve function. Histologically, affected valves may show fibrous thickening or calcification. The condition is classified under congenital heart defects and can vary in severity from mild to life-threatening. Epidemiologically, it is a rare disorder with variable prevalence rates reported in different populations. The disease course can be progressive, requiring medical or surgical intervention to prevent complications such as heart failure.
Congenital aortic valve dysplasia
Congenital aortic valve dysplasia Symptoms
Symptoms vary in severity between individuals. Early diagnosis and management can significantly improve outcomes.
Very Common
Shortness of breath manifests as difficulty in breathing, especially during physical exertion. It is caused by the reduced efficiency of the heart to pump blood due to the malformed aortic valve. Over time, this can lead to decreased exercise tolerance and increased fatigue. Patients may need to limit physical activities and may benefit from medications that improve heart function.
Chest pain occurs as a tightness or pressure in the chest, often during physical activity. It results from the heart muscle receiving insufficient oxygen due to impaired blood flow through the aortic valve. As the condition progresses, chest pain may become more frequent and severe. Patients may need to avoid strenuous activities and might require medications to manage pain and improve blood flow.
Fatigue presents as a persistent feeling of tiredness and lack of energy. It is caused by the heart's reduced ability to circulate blood efficiently, leading to decreased oxygen delivery to tissues. This symptom can worsen over time, impacting daily activities and quality of life. Management includes lifestyle modifications and medications to support cardiac function.
Common
Palpitations are experienced as a sensation of a rapid or irregular heartbeat. They occur due to the heart's compensatory mechanisms in response to inefficient blood flow through the aortic valve. Over time, palpitations can become more frequent and may indicate worsening cardiac function. Patients may find relief through medications that regulate heart rhythm.
Dizziness manifests as a feeling of lightheadedness or unsteadiness. It is caused by reduced blood flow to the brain due to impaired cardiac output. As the condition progresses, dizziness may occur more frequently, especially during physical exertion. Patients are advised to avoid sudden movements and may require medications to improve circulation.
A heart murmur is detected as an abnormal sound during a heartbeat, often identified during a physical examination. It is caused by turbulent blood flow through the malformed aortic valve. The murmur may become more pronounced as the valve dysfunction worsens. Regular monitoring and echocardiograms are essential for assessing the severity and progression of the condition.
Less Common
Swelling in the legs and ankles, known as edema, occurs due to fluid accumulation. It is caused by the heart's inability to effectively pump blood, leading to fluid retention in the lower extremities. This symptom may worsen over time, particularly in the evenings or after prolonged standing. Management includes lifestyle changes and diuretics to reduce fluid buildup.
Fainting, or syncope, is a temporary loss of consciousness often triggered by physical exertion or stress. It results from a sudden drop in blood pressure due to the heart's impaired ability to maintain adequate circulation. As the condition advances, episodes of fainting may become more frequent. Patients are advised to avoid triggers and may require treatment to stabilize blood pressure.
What Causes Congenital aortic valve dysplasia?
Congenital aortic valve dysplasia is often linked to mutations in the NOTCH1 gene, located on chromosome 9q34.3. The NOTCH1 gene encodes a transmembrane receptor involved in cell differentiation processes during cardiovascular development. Mutations in NOTCH1 can lead to misfolding of the receptor, impairing its ability to bind ligands and transmit signals. This disruption affects the Notch signaling pathway, crucial for the regulation of cell fate decisions. As a result, there is improper differentiation and proliferation of valve precursor cells, leading to structural abnormalities in the aortic valve. The malformed valve can cause altered hemodynamics, increasing stress on the heart and surrounding tissues. In response, an inflammatory process may be triggered, involving immune cells that exacerbate tissue damage. Over time, this can lead to fibrosis and calcification of the valve, contributing to its dysfunction. Neuroinflammation is not typically a primary feature, but immune responses can indirectly affect neural tissues through systemic inflammation. Degeneration of cardiac structures, such as the aortic valve, results in the characteristic symptoms of stenosis and regurgitation. Symptoms often appear as the malformed valve fails to maintain efficient blood flow, leading to heart murmurs and potential heart failure. The variability in disease severity among patients can be attributed to the specific nature of the genetic mutation, environmental factors, and the presence of modifier genes. Additionally, the extent of compensatory mechanisms in the cardiovascular system can influence symptom presentation. Understanding these molecular and cellular mechanisms is crucial for developing targeted therapies for congenital aortic valve dysplasia.
How is Congenital aortic valve dysplasia Diagnosed?
Typical age of diagnosis: Congenital aortic valve dysplasia is typically diagnosed in infancy or early childhood, often during routine pediatric examinations or when symptoms such as heart murmurs are detected. Diagnosis may also occur prenatally through fetal echocardiography if there is a known family history of congenital heart defects.
The clinician looks for signs of heart failure, such as poor feeding, tachypnea, or cyanosis, in infants. A detailed family history is crucial, especially noting any relatives with congenital heart defects. Physical examination may reveal a heart murmur, which is often the first clinical clue. This step helps determine the need for further diagnostic testing and identifies potential complications.
Echocardiography is the primary imaging modality used to assess aortic valve structure and function. It can reveal valve dysplasia, abnormal leaflet number, and associated stenosis or regurgitation. These findings confirm the diagnosis and help differentiate from other congenital heart conditions. Cardiac MRI may be used to further evaluate complex cases and exclude other structural abnormalities.
Routine blood tests may include complete blood count and metabolic panel to assess overall health. Biomarkers such as B-type natriuretic peptide (BNP) can indicate heart failure severity. Abnormal results, such as elevated BNP, guide the urgency of intervention and monitoring. These tests are supportive rather than diagnostic but help in managing the condition.
Genetic testing may involve sequencing genes such as NOTCH1, which are implicated in valve development. Mutations such as missense or nonsense variants can be identified. Positive results confirm a genetic basis for the dysplasia and guide family counseling regarding recurrence risks. This information is crucial for planning future pregnancies and understanding the condition's inheritance pattern.
Congenital aortic valve dysplasia Treatment Options
Beta-blockers are used to manage symptoms by reducing heart rate and myocardial oxygen demand. They work by blocking beta-adrenergic receptors, decreasing cardiac output. Commonly used drugs include propranolol and atenolol. Clinical evidence supports their use in reducing symptoms and improving quality of life, though they do not address the underlying valve defect. Side effects may include bradycardia, fatigue, and hypotension.
Cardiac rehabilitation involves supervised exercise programs tailored to the patient's capabilities. The goal is to improve cardiovascular fitness and reduce symptoms of heart failure. Sessions are typically held 2-3 times per week for several months. Measurable outcomes include improved exercise tolerance and reduced hospitalizations. Long-term benefits include enhanced quality of life and potentially improved survival.
Surgery is indicated for severe valve dysfunction causing significant symptoms or heart failure. The procedure involves repairing or replacing the dysplastic valve with a mechanical or bioprosthetic valve. Expected benefits include improved hemodynamics and symptom relief. Surgical risks include bleeding, infection, and valve-related complications. Post-operative care involves anticoagulation management and regular follow-up.
A team of cardiologists, nurses, dietitians, and social workers provides comprehensive care. Interventions include medication management, dietary counseling, and psychosocial support. Strategies focus on coping mechanisms and stress reduction for families. Education about the condition and its management is provided to empower families. Long-term monitoring includes regular cardiac assessments and adjustment of treatment plans as needed.
When to See a Doctor for Congenital aortic valve dysplasia
- Severe chest pain — this could indicate aortic dissection or rupture, which is a life-threatening emergency.
- Sudden shortness of breath — may suggest heart failure or severe valve obstruction requiring immediate attention.
- Loss of consciousness — could be due to insufficient blood flow to the brain, indicating critical aortic valve dysfunction.
- Persistent fatigue — may indicate worsening heart function; consult a cardiologist for evaluation.
- Palpitations or irregular heartbeat — could suggest arrhythmias associated with valve abnormalities; seek medical advice.
- Swelling in the legs or abdomen — might be a sign of heart failure; a healthcare provider should assess this.
- Mild shortness of breath during exertion — monitor for any worsening symptoms and discuss with a doctor during routine visits.
- Occasional dizziness — keep track of frequency and triggers, and report to your healthcare provider if it becomes more frequent.
Congenital aortic valve dysplasia — Frequently Asked Questions
Is this condition hereditary?
Congenital aortic valve dysplasia can have a hereditary component, often following an autosomal dominant pattern. The probability of passing the condition to children can vary depending on family history. De novo mutations can occur, meaning the condition can appear in individuals with no family history. Carrier status may not be relevant as the condition is typically expressed if inherited. Genetic counseling is recommended to understand the risks and implications for family planning.
What is the life expectancy for someone with this condition?
Life expectancy can vary significantly based on the severity and age of onset. Early diagnosis and treatment, such as valve repair or replacement, can improve outcomes. Mortality is often related to complications such as heart failure or aortic dissection. Treatment can significantly extend life expectancy and improve quality of life. Realistic expectations should be discussed with a healthcare provider, considering individual circumstances.
How is this condition diagnosed and how long does diagnosis take?
Diagnosis typically involves echocardiography, MRI, or CT scans to assess valve structure and function. The time from first symptoms to diagnosis can vary, often taking several months. Cardiologists are the primary specialists involved, but geneticists may also be consulted. Delayed diagnosis can occur due to the subtlety of early symptoms or misattribution to other conditions. Confirmation usually comes from imaging studies and sometimes genetic testing.
Are there any new treatments or clinical trials available?
Research is ongoing, with promising developments in valve repair techniques and minimally invasive procedures. Gene therapy is being explored as a potential future treatment. Clinical trials can be found on ClinicalTrials.gov by searching for congenital aortic valve dysplasia. Patients should ask their doctors about eligibility for trials and new treatments. New treatments may become available within the next decade, but timelines can vary.
How does this condition affect daily life and activities?
Mobility and self-care can be affected, especially if heart function is compromised. Educational adjustments may be necessary for children with severe symptoms. Social and emotional challenges include coping with chronic illness and potential limitations. Family burden can be significant, requiring support and resources. Adaptations such as physical therapy and support groups can help manage daily life.
Learn More
Support & Resources
References
Content generated with support from peer-reviewed literature via PubMed.
- 1.Iatrogenic or predetermined aortic dysplasia?
Wang Z, Wang Q, Zhu X · Cardiol Young · 2023 · PMID: 36805879
- 2.Congenital aortic stenosis secondary to dysplasia of congenital bicuspid aortic valves without commissural fusion.
Cheitlin MD, Fenoglio JJ Jr, McAllister HA Jr et al. · Am J Cardiol · 1978 · PMID: 677024
- 3.Pentacuspid aortic valve associated with bilateral renal artery dysplasia.
Patanè F, Ceresa F, Ferrazzo G et al. · J Cardiovasc Med (Hagerstown) · 2020 · PMID: 32332381
- 4.Bioprosthesis valve replacement in dogs with congenital tricuspid valve dysplasia: technique and outcome.
Arai S, Griffiths LG, Mama K et al. · J Vet Cardiol · 2011 · PMID: 21640677
- 5.Mucoid dysplasia of tricuspid and congenital bicuspid aortic valves in Syrian hamsters (Mesocricetus auratus).
Franco D, Durán AC, Cardo M et al. · J Comp Pathol · 1994 · PMID: 7806703
- 6.Vascular Genetics: Presentations, Testing, and Prognostics.
Aday AW, Kreykes SE, Fanola CL · Curr Treat Options Cardiovasc Med · 2018 · PMID: 30421267
- 7.The occurrence and suspected mode of inheritance of congenital subaortic stenosis and tricuspid valve dysplasia in Dogue de Bordeaux dogs.
Ohad DG, Avrahami A, Waner T et al. · Vet J · 2013 · PMID: 23434219
- 8.Congenital bicuspid aortic valve in an English bulldog.
Visser LC, Scansen BA · J Vet Cardiol · 2013 · PMID: 23434244
This content is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.Last reviewed: 2026-05-06