Immunodeficiency by defective expression of MHC class II
ih-myoo-noh-di-fi-shen-see by dee-fek-tiv eks-presh-un of MHC class two
Also known as: Bare Lymphocyte Syndrome Type II, MHC Class II Deficiency
At a Glance
What is Immunodeficiency by defective expression of MHC class II?
Immunodeficiency by defective expression of MHC class II is a rare genetic disorder that affects the immune system. It primarily impacts the body's ability to fight infections. This condition is caused by mutations in genes responsible for the expression of MHC class II molecules. Over time, affected individuals may experience recurrent infections due to the impaired immune response. Early symptoms often include frequent respiratory and gastrointestinal infections. As the condition progresses, more severe infections can occur, potentially leading to life-threatening complications. Early diagnosis is crucial to manage the condition effectively and improve outcomes. The disorder can significantly impact family life, requiring ongoing medical care and attention. Prognosis varies depending on the severity of the condition and the effectiveness of treatment. Daily life for affected individuals often involves regular medical check-ups and preventive measures to avoid infections. Treatment may include antibiotics and, in some cases, bone marrow transplantation. Support from healthcare professionals and family is essential for managing the condition.
Immunodeficiency by defective expression of MHC class II
Immunodeficiency by defective expression of MHC class II Symptoms
Symptoms vary in severity between individuals. Early diagnosis and management can significantly improve outcomes.
Very Common
Recurrent infections manifest as frequent and severe episodes of bacterial, viral, or fungal infections. This occurs due to the impaired immune response resulting from defective MHC class II expression, which is crucial for antigen presentation and activation of CD4+ T cells. Over time, these infections can lead to chronic health issues and organ damage if not properly managed. Patients often require frequent medical interventions, including antibiotics and hospitalization, to manage these infections.
Failure to thrive is observed as poor weight gain and growth in affected children. The underlying cause is the body's inability to effectively fight infections and absorb nutrients due to chronic illness. As the condition progresses, it can lead to developmental delays and nutritional deficiencies. Nutritional support and management of infections are essential to improve growth outcomes.
Chronic diarrhea presents as persistent loose or watery stools. It is often caused by gastrointestinal infections or malabsorption issues due to the compromised immune system. If left untreated, it can lead to dehydration, electrolyte imbalances, and malnutrition. Management includes rehydration, dietary adjustments, and treatment of underlying infections.
Common
Lymphopenia is characterized by a reduced number of lymphocytes in the blood. This occurs because of impaired development and function of T cells due to defective MHC class II expression. Over time, lymphopenia contributes to the increased susceptibility to infections. Regular monitoring and immune-boosting therapies can help manage this condition.
Hepatosplenomegaly is the enlargement of the liver and spleen. It results from the accumulation of immune cells and ongoing immune activation due to chronic infections. This condition can cause abdominal discomfort and affect normal organ function. Treatment focuses on managing underlying infections and monitoring organ size.
Autoimmune manifestations can include symptoms such as skin rashes or joint pain. These occur when the immune system mistakenly attacks the body's own tissues, a risk increased by immune dysregulation. Over time, these symptoms can lead to chronic pain and tissue damage. Immunosuppressive therapies may be required to control autoimmune activity.
Less Common
Neurological symptoms may include developmental delays or seizures. These arise due to the potential impact of chronic infections and immune dysregulation on the nervous system. If not addressed, they can lead to long-term cognitive and motor impairments. Early intervention with therapies and medications can help manage these symptoms.
Skin infections manifest as recurrent or persistent rashes, boils, or abscesses. The impaired immune response allows for opportunistic infections to affect the skin more frequently. Without proper treatment, these infections can become severe and lead to scarring. Topical and systemic antimicrobial treatments are often necessary to control skin infections.
What Causes Immunodeficiency by defective expression of MHC class II?
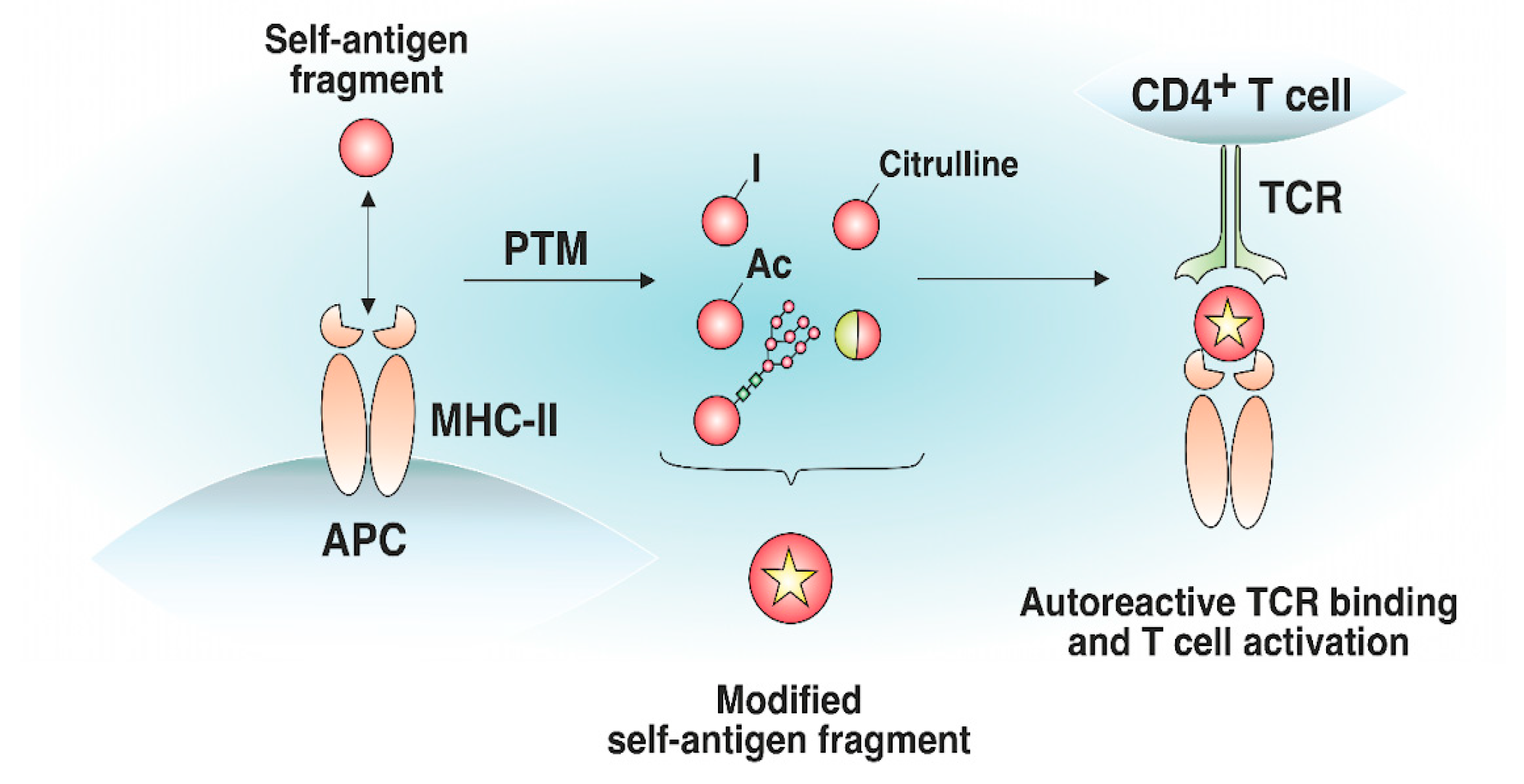
Immunodeficiency by defective expression of MHC class II is primarily caused by mutations in the CIITA, RFXANK, RFX5, and RFXAP genes, which are located on chromosomes 16, 19, 1, and 13 respectively. These genes encode transcription factors that are crucial for the expression of MHC class II molecules on the surface of antigen-presenting cells. Mutations in these genes can lead to defective transcriptional activation of MHC class II genes, resulting in the absence or reduced expression of MHC class II molecules. This molecular defect impairs the presentation of antigenic peptides to CD4+ T cells, leading to a failure in the activation and proliferation of these cells. Consequently, the immune response is severely compromised, as CD4+ T cells play a pivotal role in orchestrating the adaptive immune response. The lack of MHC class II expression causes a cascade of immune dysfunction, affecting neighboring immune cells such as B cells and macrophages. This disruption can lead to neuroinflammation due to the inability to regulate immune responses effectively, potentially affecting the central nervous system. White matter degeneration may occur as a result of chronic inflammation and immune dysregulation, which can damage neural tissues. Symptoms typically manifest as recurrent infections, failure to thrive, and developmental delays, reflecting the critical role of CD4+ T cells in immune surveillance and response. The variability in disease severity among patients is often due to the specific gene affected, the nature of the mutation, and the residual activity of the transcriptional machinery. In some cases, partial expression of MHC class II molecules may occur, leading to milder phenotypes. Environmental factors and additional genetic modifiers can also influence the clinical presentation and progression of the disease. Understanding the precise genetic and molecular mechanisms underlying this condition is essential for developing targeted therapies and improving patient outcomes.
How is Immunodeficiency by defective expression of MHC class II Diagnosed?
Typical age of diagnosis: Diagnosis typically occurs in early childhood, often before the age of 5, when recurrent infections and failure to thrive prompt further investigation. Initial suspicion arises from clinical presentation and family history of immunodeficiency disorders.
The clinician looks for signs of recurrent infections, growth retardation, and failure to thrive. A detailed family history of immunodeficiency disorders is crucial in guiding suspicion. Physical examination may reveal lymphoid tissue hypoplasia and skin infections. This step helps shape the diagnostic direction towards immunological disorders.
Chest X-rays or CT scans are used to assess the presence of chronic lung infections or structural abnormalities. Specific abnormalities such as bronchiectasis or lymphoid tissue hypoplasia may be visible. These findings can support the diagnosis of an immunodeficiency disorder. Imaging helps exclude differentials like cystic fibrosis or primary ciliary dyskinesia.
Flow cytometry is ordered to assess lymphocyte subsets and function. Biomarkers such as low CD4+ T-cell counts and absent HLA-DR expression are sought. Abnormal results include reduced or absent MHC class II expression on B cells and monocytes. These results guide the next steps towards genetic testing for confirmation.
Genes such as CIITA, RFXANK, RFX5, and RFXAP are sequenced. Mutations like point mutations, deletions, or insertions are found. Results confirm the diagnosis by identifying specific genetic defects causing MHC class II deficiency. Genetic testing informs family counseling regarding carrier status and recurrence risks.
Immunodeficiency by defective expression of MHC class II Treatment Options
This therapy involves the use of intravenous or subcutaneous immunoglobulins. It works by providing passive immunity to reduce the frequency and severity of infections. Specific products include IVIG and SCIG, which have shown efficacy in reducing infection rates. Clinical evidence supports its use in improving quality of life and reducing hospitalizations. Limitations include potential side effects like allergic reactions and the need for regular infusions.
Techniques such as chest physiotherapy and breathing exercises are used. The therapeutic goal is to improve lung function and clear respiratory secretions. Sessions are typically conducted several times a week, lasting 30-60 minutes each. Measurable outcomes include improved pulmonary function tests and reduced respiratory infections. Long-term benefits include enhanced respiratory health and quality of life.
Indicated for severe cases with life-threatening infections. The procedure involves replacing defective immune cells with healthy donor stem cells. Expected benefits include the restoration of normal immune function and reduced infection rates. Surgical risks include graft-versus-host disease and infection. Post-operative care requires immunosuppression and monitoring for complications.
The team includes immunologists, infectious disease specialists, and nutritionists. Specific interventions include infection prophylaxis, nutritional support, and regular monitoring. Psychosocial support strategies involve counseling and support groups for patients and families. Family education focuses on infection prevention and recognizing early signs of complications. Long-term monitoring plans include regular follow-ups and immunological assessments.
When to See a Doctor for Immunodeficiency by defective expression of MHC class II
- Severe recurrent infections — this indicates a significant immune system dysfunction requiring immediate medical attention.
- Failure to thrive in infants — this can lead to developmental delays and requires urgent evaluation.
- Respiratory distress — this can be life-threatening and needs emergency intervention.
- Chronic diarrhea — may indicate malabsorption issues and requires medical evaluation.
- Persistent skin rashes — could signify an underlying immune problem and should be assessed by a healthcare provider.
- Delayed growth milestones — may suggest underlying health issues and warrants further investigation.
- Mild recurrent colds — monitor frequency and duration, and consult a doctor if they worsen.
- Occasional fatigue — track energy levels and consult a healthcare provider if it becomes more frequent or severe.
Immunodeficiency by defective expression of MHC class II — Frequently Asked Questions
Is this condition hereditary?
This condition is typically inherited in an autosomal recessive pattern. This means both parents must carry a copy of the mutated gene to pass it on to their child. De novo mutations are rare but can occur. Carriers usually do not show symptoms but can pass the condition to their children. Genetic counseling is recommended for affected families to understand risks and implications.
What is the life expectancy for someone with this condition?
Life expectancy varies significantly based on the age of onset and severity of symptoms. Early diagnosis and treatment can improve outcomes and extend survival. Mortality is often due to severe infections or complications from immune deficiency. Treatment, including bone marrow transplantation, can significantly improve survival rates. Realistic expectations should include ongoing medical care and monitoring.
How is this condition diagnosed and how long does diagnosis take?
Diagnosis involves genetic testing and immunological assessments to confirm MHC class II deficiency. The time from first symptoms to diagnosis can vary, often taking months to years due to symptom overlap with other conditions. Immunologists and geneticists are typically involved in the diagnostic process. Delays often occur due to the rarity of the condition and lack of awareness. Confirmation is achieved through genetic testing identifying mutations in relevant genes.
Are there any new treatments or clinical trials available?
Current research is exploring gene therapy as a promising treatment for MHC class II deficiency. Novel approaches aim to correct the underlying genetic defects. ClinicalTrials.gov is a resource for finding relevant trials, and patients should discuss potential participation with their doctors. It's important to ask about the risks and benefits of new treatments. While promising, these treatments may take years before becoming widely available.
How does this condition affect daily life and activities?
The condition can significantly impact mobility and self-care due to frequent infections and hospitalizations. Educational challenges may arise from missed school and cognitive impacts. Social and emotional challenges include isolation and anxiety related to health issues. Family burden can be substantial, requiring adjustments and support. Supportive therapies and accommodations at school and home can help manage these challenges.
Learn More
Support & Resources
References
Content generated with support from peer-reviewed literature via PubMed.
- 1.HLA-DR covers Bare Lymphocyte Syndrome.
Yadav RM, Bargir UA, Ganapule A et al. · Scand J Immunol · 2021 · PMID: 32875602
- 2.A Spontaneous H2-Aa Point Mutation Impairs MHC II Synthesis and CD4(+) T-Cell Development in Mice.
Zhao Y, Xiong J, Chen HX et al. · Front Immunol · 2022 · PMID: 35309308
- 3.A large single-center cohort of bare lymphocyte syndrome: Immunological and genetic features in Turkey.
Ünsal H, Caka C, Bildik HN et al. · Scand J Immunol · 2024 · PMID: 38441205
- 4.[A major histocompatibility complex class Ⅱ deficiency case report and literature review].
Wu WC, Wang W, Song HM et al. · Zhonghua Er Ke Za Zhi · 2016 · PMID: 27510876
- 5.Novel variants in CIITA caused type II bare lymphocyte syndrome: A case report.
Zhang Y, Yokoyama Y, Qing Y et al. · Asian Pac J Allergy Immunol · 2024 · PMID: 33386785
- 6.Lessons learned from the diagnostic work-up of a patient with the bare lymphocyte syndrome type II.
Damoiseaux M, Damoiseaux J, Pico-Knijnenburg I et al. · Clin Immunol · 2022 · PMID: 35065305
- 7.A novel mutation in RFXANK gene and low B cell count in a patient with MHC class II deficiency: a case report.
Abolnezhadian F, Dehghani R, Dehnavi S et al. · Immunol Res · 2020 · PMID: 32578129
- 8.Major Histocompatibility Complex Class II Deficiency due to a Novel Mutation in RFXANK in a Child of Mexican Descent.
Clarridge K, Leitenberg D, Loechelt B et al. · J Clin Immunol · 2016 · PMID: 26634365
This content is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.Last reviewed: 2026-05-09